Trigger Points and Treatment Modalities
Summary
In this compilation we delve into the idea of “trigger points” and the modalities used to treat this phenomenon (myofascial release, acupuncture/dry needling, cupping, TENS, placebo). The explanation of muscular trigger points themselves, presented by alternative healthcare practitioners, is highly controversial and unable to be validated by current research. Many of the modalities for treatment appear to depend on the placebo effect or function as a palliative measure only.
Currently, it appears that treatment modality is interchangeable from an efficacy standpoint, even with sham treatments. To quote Mikkelsen: “The problem is not that nothing works. The problem is that anything can work.”
Further research is needed into these areas to make definitive conclusions as the evidence is generally of very low quality.
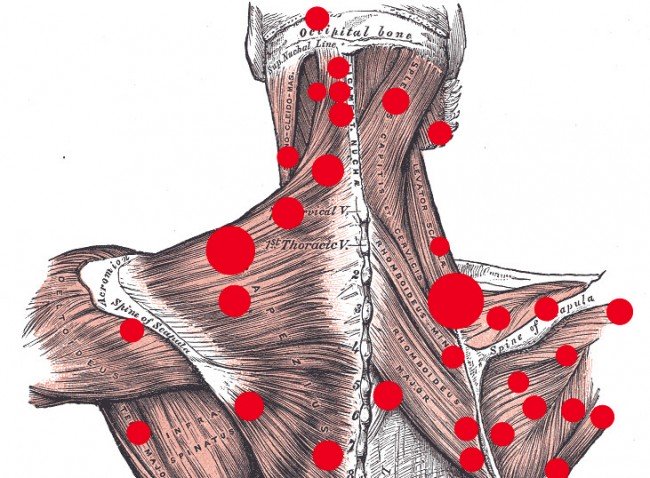
The theory of myofascial pain syndrome caused by muscular trigger points has been refuted. This is not to deny the existence of the clinical phenomena themselves, for which scientifically sound and logically plausible explanations can be advanced.
Potential culprits for “trigger points” are issues with the axons of peripheral nerves, central nervous system over-stimulation, subjective experience with subsequent sensitization to danger signalling, or simply confirmation bias. There is quite a lot of debate over the nociceptive and CNS components of pain, especially in chronic pain conditions. Research routinely shows physical phenomena does not always match up with the subjective experience of pain. This does not mean that nociceptive/CNS influence isn’t a factor, only that it is not always necessary. Based on current evidence, pain is an experience of danger signalling modified by the individual’s perception. Keeping this in mind, addressing physical causes as well as providing adjunct educational therapies is warranted in persistent pain cases.
Myofascial Release

Muscular “knotting” has not currently been confirmed by credible research. Regardless, deep muscular tissues are not affected by myofascial manipulation. Therefore, the concept of working out “knots” is not only controversial, it is not backed by distinct clinical evidence. Additionally, there is no evidence that the use of modalities such as lacrosse ball massage, trigger point massage, Theraguns, or foam rolling will provide benefits such as clearing up lactic acid or changing sarcomere length.
There is insufficient evidence to support that the primary mechanisms underlying rolling and other similar devices are the release of myofascial restrictions and thus the term “self-myofascial release” is misleading.Behm and Wilke 2019
There are many myths surrounding myofascial issues and the benefits of treatment:
- “Increased circulation”: despite the fact that this has never been shown consistently in the research, minute changes would be trivial anyway. Being active (walking, jogging, any physical activity really) improves circulation better than any of these therapies ever could.
- “Detoxification”: No. Stop. If anything, massage interferes with elimination of toxins.Wiltshire et al 2010
- “Cortisol”: There is no scientific consensus on this.
- “Tight Muscles”: Therapists accept this because of a phenomenon called palpatory pareidolia. The idea that a vague perception is accepted as real. When blinded, therapists have not reliably been able to palpate and predict these areas of pain or tightness in patients in trials.
- “Delayed Onset Muscle Soreness or DOMS”: Massage has been shown to both increase and decrease post-exercise soreness. Torres et al 2012
Crane 2012 is often misinterpreted as showing that massage helps alleviate DOMS and inflammation. The results of this study were actually negative: the data showed that massage has no significant effect on gene expression in muscle cells. Ingraham remarks: “There are several major problems with the study: the sample size was extremely small; the number of changes they found was trivial (and dwarfed by what exercise causes); the size of the differences was barely statistically significant—and short-lived, too; they measured genetic “signals” and not actual results, and guessed about their meaning; and we already know from clinical trials that massage doesn’t work any miracles for soreness after exercise, so what is there for the data to “explain”?”
- “Endorphins”: “We found no significant pretreatment or posttreatment difference in blood beta-endorphin or beta-lipotropin levels between the groups. The results indicate that massage did not change significantly the measured serum levels of beta-endorphin or beta-lipotropin” Day et al 1987
- “Inflammation”: Strong massage modestly damages tissues. If anything it promotes inflammation slightly. See above for explanation of the Crane 2012 results.
Crane 2012 is often misinterpreted as showing that massage helps alleviate DOMS and inflammation. The results of this study were actually negative: the data showed that massage has no significant effect on gene expression in muscle cells. Ingraham remarks: “There are several major problems with the study: the sample size was extremely small; the number of changes they found was trivial (and dwarfed by what exercise causes); the size of the differences was barely statistically significant—and short-lived, too; they measured genetic “signals” and not actual results, and guessed about their meaning; and we already know from clinical trials that massage doesn’t work any miracles for soreness after exercise, so what is there for the data to “explain”?”
If massage works, it’s mainly because of the neurology of touch, as opposed to changing tissues. Ingraham 2018
People receive comfort through touch. Like every other modality in alternative medicine, the research is extremely poor and treatments have not been substantiated beyond placebo (the most glaring issues being a lack of blinding in the larger studies which could lead to a reverse placebo effect and/or conclusions that are contradictory to the evidence presented). Ultimately, massage may simply work because it is relaxing. Shulman 1996
Dry Needling & Acupuncture
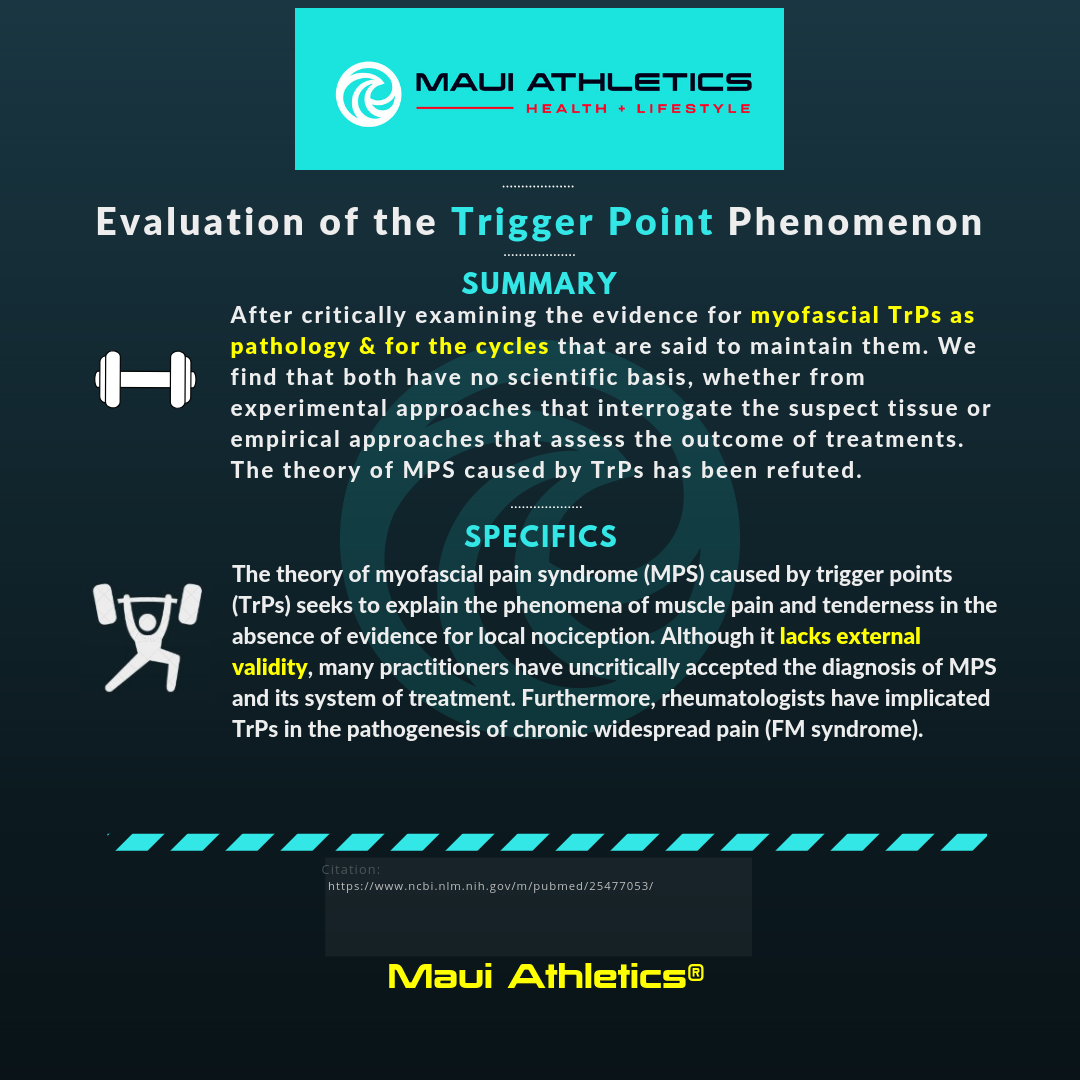
The research for dry needling and acupuncture is varied. Some suggest better results than no treatment, whereas others do not. Much of the research suggests similar results to sham needling. Dry-needlists tend to have 48-72 hours of training on average and in many states are not required to have any license or training at all to perform their craft. Acupuncturists tend to have much more strict licensing and training that requires over a year of study.
Some of the systemic reviews and meta analyses that did not select for blinded trials were not included in the article due to this majorly confounding variable. Not only is placebo a concern, but a reverse placebo effect has been seen in those that are known to be control subjects.

Dry-needling/acupuncture was not found to be significantly superior to placebo in this meta-analysis.
This meta-analysis found no difference in functional outcome exists when compared to other physical therapy treatments. Evidence of long-term benefit of dry needling is currently lacking.
“Serious adverse events (AEs) related to acupuncture are rare, but need significant attention as mortality can be associated with them. Referrals should consider acupuncturists’ training credibility, and patient safety should be a core part of acupuncture education.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5469776/
This systemic review states: “We conclude there is limited evidence that acupuncture is more effective than no treatment for chronic pain; and inconclusive evidence that acupuncture is more effective than placebo, sham acupuncture or standard care.”
https://www.ncbi.nlm.nih.gov/pubmed/10812251
This systemic review states: “Acupuncture probably has little or no effect in reducing pain or improving function relative to sham acupuncture in people with hip osteoarthritis. Due to the small sample size in the studies, the confidence intervals include both the possibility of moderate benefits and the possibility of no effect of acupuncture.”
https://www.ncbi.nlm.nih.gov/pubmed/29729027
“In conclusion, there is limited evidence deriving from one study that deep needling directly into myofascial trigger points has an overall treatment effect when compared with standardised care. Whilst the result of the meta-analysis of needling compared with placebo controls does not attain statistically significant”
https://www.ncbi.nlm.nih.gov/pubmed/18395479
TENS
Data is too poor to draw a conclusion, but it is not overly promising.

Photo adapted from Ingraham
Cupping
High quality studies have never shown an objective measure of pain relief or other benefit to cupping, on the contrary, they show no benefit. The studies that do show positive outcomes tend to be of low quality and of subjective measure. There may be concern regarding the use of cupping in those with eczema in particular.
Essentially, cupping damages skin and the underlying blood vessels. I do not recommend it as a treatment as cupping has even been implicated in 3rd degree burns and sepsis (along with other serious damage to tissue).
Systemic reviews that did not control for type of cupping or condition of the patient were not included as the better systemic reviews that have been included were of poor enough quality as is.
“Currently there are few RCTs testing the effectiveness of cupping in the management of pain. Most of the existing trials are of poor quality. Therefore, more rigorous studies are required before the effectiveness of cupping for the treatment of pain can be determined.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136528/
“Cupping therapy can significantly decrease the VAS scores and ODI scores for patients with LBP compared to the control management. High heterogeneity and risk of bias existing in studies limit the authenticity of the findings.”
https://www.ncbi.nlm.nih.gov/pubmed/28946531
This systemic review found: “No explicit recommendation for or against the use of cupping for athletes can be made.”
https://www.ncbi.nlm.nih.gov/pubmed/29185802
This systemic review and meta-analysis found: “Only weak evidence can support the hypothesis that cupping therapy can effectively improve the treatment efficacy and physical function in patients with knee osteoarthritis.”
https://www.ncbi.nlm.nih.gov/pubmed/28779923
Placebo
Interestingly enough, many researchers and physiotherapists understand that these treatments are potentially bunk. Placebo itself may be driving the subjective benefits. This does produce some ethical dilemmas regarding the use of these treatments. Even when a patient is informed of the lack of scientific backing, there may be exacerbation of the chronic pain condition if these treatments are used instead of focusing on education.
“Placebo is traditionally considered an inert intervention; however, the pain research literature suggests that placebo is an active hypoalgesic agent. Placebo response likely plays a role in all interventions for pain and we suggest that the same is true for the treatment effects associated with manual therapy. The magnitude of a placebo response may be influenced by negative mood, expectation, and conditioning. We suggest that manual therapists conceptualize placebo not only as a comparative intervention, but also as a potential active mechanism to partially account for treatment effects associated with manual therapy. We are not suggesting manual therapists include known sham or ineffective interventions in their clinical practice, but take steps to maximize placebo responses to reduce pain.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3172952/
![]()




